What is Meningoencephalomyelitis of Unknown Etiology (MUE)?
MUE is a presumptive immune-mediated disease, which results in inflammation within the brain or spinal cord. Inflammation within the brain is called encephalitis; inflammation within the spinal cord is called myelitis; inflammation within the lining of the spinal cord and the brain is called meningitis. The most common form of MUE is granulomatous meningoencephalomyelitis (GME) hence these terms being used interchangeably in this review.

The immune system should normally function to help protect the body from things like infections, but in dogs and cats with MUE, the immune system starts to attack the brain and the spinal cord.
MUE / GME can be focal (only affecting one part of the brain or spinal cord) or it can be multi-focal (affecting multiple areas of the brain and/or spinal cord). There is also a form of MUE / GME (called Optic Neuritis), which only affects the nerves to
the eyes.

What Clinical Signs Occur with MUE?
Dogs with MUE can have a range of clinical signs. Some animals will have only back or neck pain. Some have seizures, behavioral changes, blindness, and balance issues. Some animals have difficulty walking, have an uncoordinated gait, or lose
the ability to walk or move their limbs (paralysis).
Which Animals are Prone to Developing MUE/GME?
MUE occurs most commonly in young to middle-aged dogs. Female dogs are more prone to development of disease. Certain dog breeds tend to develop MUE more than others, and this includes Maltese, Yorkshire Terriers, Pugs, Miniature Poodles,
and Chihuahuas.
While MUE tends to affect young, female, toy breed dogs, it is important to keep in mind that any age, sex, or breed can develop MUE.
What Causes MUE / GME?
The underlying cause of MUE / GME is unknown, but there are several theories, including genetic causes, a primary autoimmune disease, and infectious triggers.
There seems to be a genetic predisposition for the development of MUE given that there are common breeds affected. Female dogs also seem to be predisposed, which is similar to autoimmune diseases in people (like multiple sclerosis).
There have been multiple studies looking for a common infectious cause of MUE, but testing for many viral causes, bacterial causes, and tick-borne diseases have all failed to identify a consistent infectious agent.
Ultimately, we still don’t know the true cause of MUE. Most believe it is a nonspecific response of the immune system, but multiple environmental triggers and genetic factors probably play a role in the development of the disease.
How is MUE Diagnosed?
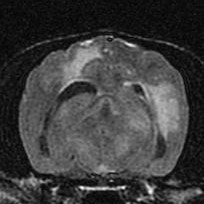
The first step is usually to perform an MRI of the brain and/or spinal cord. Animals with MUE usually have areas of inflammation in the brain or spinal cord, which can be seen with an MRI. It is also possible that animals with MUE can have a normal MRI.

The second step is to perform a spinal tap to collect spinal fluid. The spinal fluid is sent to a laboratory for analysis. Most animals with MUE have an increased white blood cell count (pleocytosis) and protein level in their spinal fluid. Rarely, sometdogs with MUE will have a normal spinal fluid analysis; this tends to happen most commonly in animals who are already receiving steroid medications. It is also sometimes helpful to have a Clinical Pathologist review slides of the spinal fluid to help identify which type of white blood cells are increased. The types of white blood cells that are increased can help us decide whether the changes we see on MRI and in the spinal fluid are most consistent with MUE or consistent with an infection.
For certain cases, it may be important to rule-out possible infectious causes of the inflammation within the brain and/or spinal cord. Infectious causes of inflammation include a viral infection (like Distemper virus), a fungal infection (like Cryptococcus), a protozoal infection (like Toxoplasmosis or Neosporosis), a tickborne infection (like Rocky Mountain Spotted Fever or Ehrlichiosis), and a bacterial infection (like from a distant or adjacent source that spreads to the brain or spinal cord). The decision on whether to submit samples for infectious disease testing is based on the results of the MRI and spinal tap, and it also based on whether or not your pet is a “typical” breed of dog that commonly develops MUE.
Ultimately, the only way to definitively diagnose MUE is with a surgical biopsy of the brain. However, since we can typically make a confident diagnosis based on your pet’s breed, age, MRI findings, and spinal fluid findings, a brain biopsy is usually not clinically necessary.
How is MUE / GME Treated?
Since MUE is a disorder of the immune system, it is treated by using medications to help suppress the abnormal response of the immune system. Decreasing the abnormal immune response will help to decrease the inflammation within the brain and/or the spinal cord.
The abnormal immune response is usually (and best) treated with a combination of medications. The medications used can vary based on the best fit for you and your pet, but the most common combination of medications that we use is Prednisone (or Prednisolone), Cyclosporine, and Cytarabine / Cytosar. Sometimes we may use other medications to suppress the immune system, like Leflunomide, CCNU, or Azathioprine.
Prednisone or Prednisolone is a steroid that helps suppress the immune system. Side effects of this medication include an increased appetite, increased thirst, increased urination, and increased panting. Sometimes Prednisone can cause gastrointestinal ulcerations or bleeding. This medication is usually given for the rest of your pet’s life; however, we try to taper the dose of Prednisone to the lowest dose possible that will still control clinical signs. This tapering of Prednisone is
usually done very slowly (over many months).
Cytarabine is a chemotherapy medication that specifically targets inflammation in the brain and spinal cord. Side effects are relatively rare with this drug, and it is usually very well tolerated. The most commonly reported side effect we worry about the most is a decreased white blood cell count in the blood. A low white blood cell count could potentially predispose your pet to an infection (urinary tract infection, pneumonia, skin infection). Initially, we may monitor your pet’s complete blood count (CBC) 7-10 days after each round of injections. Over time, we may be able to decrease how often we perform a CBC. Vomiting, diarrhea, or a decreased appetite can occur with Cytarabine, but most dogs do not have any noticeable
adverse effects.
Cytarabine is usually given as an injection under the skin over a one- or two-day period. We usually administer the medication every 3-4 weeks for 6 months, but after that round of therapy, the injections can sometimes be spaced out to once every five or six weeks.
What is the Prognosis for MUE / GME?
In general, MUE is not curable, and most pets require life-long treatment. The goal of treatment is to get your pet back to living as normal of a life as possible, and it is very possible that your pet will return to a neurologically normal state. Recurrence of neurologic signs is possible even during treatment. If this occurs, we will have to modify the medications that your pet is receiving.
The prognosis for GME in one study looking at dogs treated with a combination of Prednisone and Cytarabine was 531 days. However, this is an average survival time, and some dogs live much longer, and some dogs live much shorter time
periods. In our experience, approximately 70% of dogs respond favorably to treatment and clinically do well long-term.
References
- Talarico LR, Schatzberg SJ. Idiopathic granulomatous and necrotising inflammatory disorders of the canine central nervous system: a review and future perspectives. JSAP 2010; 51, 138-149.
- Barber RM, Li Q, Diniz PP. Evaluation of brain tissue or CSF with broadly reactive PCR for Ehrlichia, Anaplasma, spotted fever group Rickettsia, Bartonella, and Borrelia species in canine neurological diseases (109 cases). JVIM 2010; 24(2), 372-8.
- Barber RM, Porter BF, Li Q. Broadly reactive PCR for pathogen detection in canine GME and NME. JVIM 2012; 26(4), 962-8.
- Greer KA, Schatzberg SJ, Porter BF. Heritability and transmission analysis of NME in the Pug. Res Vet Sci 2009; 86(3), 438-42.
- Herrera BM, Cader MZ, Dyment DA. Multiple sclerosis susceptibility and the X chromosome. Multiple Sclerosis 2007; 13, 856-64.
- Hoffman GE, Le WW, Murphy AZ. Divergent effects of ovarian steroids on neuronal survival during experimental allergic encephalitis in Lewis rats. Experimental Neurology 2001; 171, 272-84.
- Jurney CH, Van Winkle TJ, Shofer FS, et al. Necrotizing encephalitis: A retrospective study of 36 cases. JVIM 2007; 21:641.
- Levine JM, Fosgate GT, Porter B, et al. Epidemiology of Necrotizing Meningoencephalitis in Pug Dogs.
- Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Molecular and Cellular Endocrinology 2011;335:2-13.
- Menaut P, Landart J, Behr S, et al. Treatment of 11 dogs with MUE with a combination of prednisone and cytosine arabinoside. Vet Record 2008; 162:241-245.
- Zarfoss M, Schatzberg S, Venator K, et al. Combined cytosine arbinoside and prednisone therapy for MUE in 10 dogs. JSAP 2006;47:588-595.
- Adamo PF, Rylander H, Adams WM. Ciclosporin use in multi-drug therapy for MUE in dogs. JSAP 2007;48:486-496.
- Flegel T, Boettcher IC, Matiasek K, et al. Comparison of oral administration of lomustine and prednisilone or prednisilone alone as treatment for GME or NE in dogs. JAVMA 2011;238:337-345.
- Gregory CR, Stewart A, Sturges B, et al. Leflunomide effectively treats naturally occurring immune-mediated and inflammatory diseases of dogs that are unresponsive to conventional therapy. Transplantation Proceedings 1998;30:4143-4148.
- Munana KR, Luttgen PJ. Prognostic factors for dogs with GME: 42 cases (1982-1996). JAVMA 1998;212:1902-1906.
- Coates JR, Barone G, Dewey CW, et al. Procarbazine as adjunctive therapy for treatment of dogs with presumptive antemortem diagnosis of GME: 21 cases. JVIM 2007;21:100-106.
- Granger N, Smith PM, Jeffery ND. Clinical findings and treatment of non-infecious meningoencephalomyeitis in dogs: A systematic review of 457 published cases. Vet Journal 2010;184:290-297.